Adenomyosis vs fibroids is a common source of confusion for women experiencing heavy periods, pelvic pain, bloating, or pressure in the lower abdomen. Although both benign uterine conditions can cause similar symptoms, they affect the uterus differently and may require different treatment plans.
Heavy bleeding, severe cramps, anemia, and pelvic discomfort can affect work, relationships, sleep, and emotional wellbeing.
When symptoms are dismissed as “normal periods,” diagnosis may be delayed and women may continue living with avoidable pain and exhaustion.
Accurate imaging, a complete gynecological assessment, and a personalized treatment plan can help identify whether adenomyosis, uterine fibroids, endometriosis, or a combination of conditions is responsible.

Adenomyosis vs Fibroids: What Is the Difference?
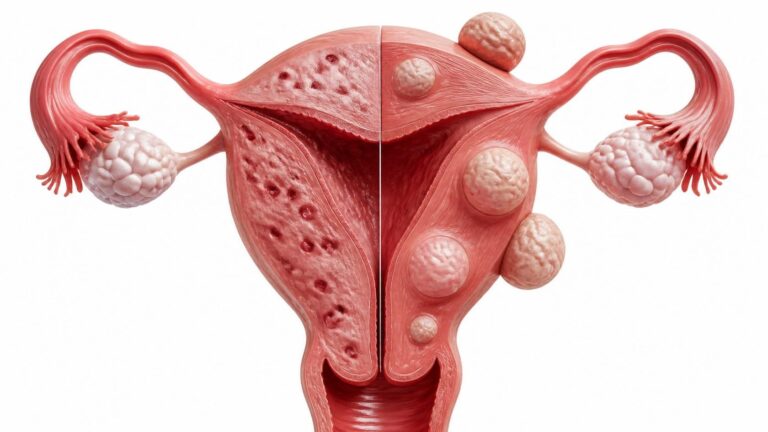
Adenomyosis grows within the muscular wall of the uterus, while fibroids are distinct solid, noncancerous growths that develop from uterine muscle tissue.
Adenomyosis occurs when tissue similar to the uterine lining, called endometrial tissue, grows into the myometrium, the muscle layer of the womb. This can make the uterus enlarged, tender, and more likely to cause painful or heavy menstrual bleeding.
Uterine fibroids, also called leiomyomas or myomas, are solid growths made of muscle and fibrous tissue. They can develop inside the uterine cavity, within the uterine wall, or on the outer surface of the uterus.
| Feature | Adenomyosis | Uterine Fibroids |
| Main location | Within the uterine muscle wall | Inside, within, or outside the uterine wall |
| Tissue type | Endometrial glands and tissue in muscle | Smooth muscle and fibrous tissue |
| Appearance | Diffuse or focal thickening of the uterus | Distinct, rounded solid masses |
| Common symptoms | Painful, heavy periods and pelvic tenderness | Heavy bleeding, pressure, bloating, urinary symptoms |
| Uterus shape | Often uniformly enlarged | May appear irregular or lumpy |
| Fertility impact | May affect implantation and pregnancy in some women | Depends on fibroid size and location |
| Minimally invasive options | Selected embolization-based approaches | Uterine artery embolization and selected image-guided treatments |
Adenomyosis and fibroids are not cancer, but both conditions can significantly affect reproductive health, daily life, and quality of life. Research confirms that they may occur together, making professional diagnosis especially important.
What Are the Main Symptoms of Adenomyosis vs Fibroids?
Adenomyosis more often causes severe menstrual cramps and a tender uterus, while fibroids more commonly cause pressure symptoms, visible abdominal enlargement, and heavy bleeding.
Both conditions can cause abnormal uterine bleeding, painful periods, pelvic heaviness, and iron-deficiency anemia. However, their symptom patterns often provide useful clues.
Common adenomyosis symptoms include:
- Heavy or prolonged menstrual bleeding
- Severe cramping during periods
- Deep pelvic pain or pressure
- Pain during intercourse
- A tender, enlarged uterus
- Pelvic discomfort that worsens before or during menstruation
- Fatigue related to anemia
Common uterine fibroid symptoms include:
- Heavy menstrual bleeding or passing large clots
- Pelvic pressure or fullness
- Abdominal enlargement or bloating
- Frequent urination from bladder pressure
- Constipation from pressure on the bowel
- Lower back discomfort
- Difficulty becoming pregnant in selected cases
Recent studies indicate that symptom severity does not always match the size of a fibroid. A small fibroid inside the uterine cavity may cause substantial bleeding, while a larger fibroid on the outer uterine surface may cause pressure with little menstrual disruption.
How Is Adenomyosis vs Fibroids Diagnosed?
Transvaginal ultrasound is usually the first imaging test for adenomyosis and fibroids, while MRI can clarify difficult or mixed cases.
Diagnosis starts with a detailed medical history, including bleeding pattern, pain severity, fertility goals, previous surgery, medication use, and family history. A pelvic examination may identify an enlarged, tender, irregular, or bulky uterus.
Doctors recommend a transvaginal ultrasound because it can assess the uterine wall, endometrial cavity, ovaries, and the presence of fibroids. It is often the first step when heavy menstrual bleeding, painful periods, pelvic pain, or reproductive concerns occur.
MRI may be useful when ultrasound findings are unclear or when adenomyosis, adenomyomas, fibroids, and endometriosis may coexist. MRI can provide more detailed information about the thickness and structure of the uterine wall and help guide treatment planning.
Blood tests may also be needed to assess anemia, iron deficiency, thyroid abnormalities, pregnancy, or other causes of abnormal bleeding. In some women, hysteroscopy or endometrial sampling may be recommended to investigate abnormal bleeding or rule out other uterine conditions.
Can Adenomyosis vs Fibroids Be Seen on Ultrasound?
Yes, ultrasound can often distinguish adenomyosis from fibroids, but the two conditions can overlap and MRI may be needed for a clearer diagnosis.
Fibroids usually appear as well-defined, solid, rounded masses. Their location is important because submucosal fibroids, which grow toward the uterine lining, often cause heavy bleeding and fertility problems.
Adenomyosis may appear as a thickened, uneven, or heterogeneous uterine muscle wall. Ultrasound features can include small cystic spaces within the myometrium, an irregular junction between the uterine lining and muscle, fan-shaped shadowing, and asymmetrical wall thickening.
Can adenomyosis look like fibroids on ultrasound? Yes. Focal adenomyosis, sometimes called an adenomyoma, can resemble a fibroid because it may form a localized area of thickened muscle. Unlike a typical fibroid, however, an adenomyoma often has less distinct borders.
According to available medical evidence, imaging should always be interpreted alongside symptoms, examination findings, and reproductive goals. A normal scan does not automatically explain severe pain, especially if endometriosis or another pelvic disorder is also possible.
What Are the Treatment Options for Fibroid and Adenomyosis?
Treatment for fibroids and adenomyosis depends on symptoms, anemia, fibroid location, age, fertility plans, and whether the patient wants to preserve the uterus.
Mild symptoms may be managed with observation, iron treatment for anemia, anti-inflammatory medications, tranexamic acid for heavy bleeding, or hormone-based therapy. Hormonal options may include combined hormonal contraception, progestogen therapy, or a levonorgestrel-releasing intrauterine system where suitable.
Some women may be offered medications that temporarily reduce estrogen activity. LUPRON DEPOT is a gonadotropin-releasing hormone agonist that may be used in specific clinical situations, including short-term management before fibroid surgery in selected patients with anemia. Its Safety Information and suitability must be reviewed individually because hormone-suppressing therapy can have side effects and is not a permanent solution.
For fibroids, treatment options may include:
- Medication to control bleeding or pain
- Hysteroscopic treatment for selected fibroids inside the uterine cavity
- Myomectomy to remove fibroids while preserving the uterus
- Uterine artery embolization
- Hysterectomy when other treatments are unsuitable or have failed
For adenomyosis, options may include:
- Pain relief and anti-inflammatory medication
- Hormonal therapy
- Levonorgestrel intrauterine system
- Selected image-guided embolization treatment
- Surgical management in severe cases
Dr. Samir Abdel Ghaffar, Consultant Interventional Radiologist, evaluates women with symptomatic uterine fibroids and selected adenomyosis cases using advanced imaging and minimally invasive interventional radiology techniques. His approach focuses on reducing symptoms while preserving the uterus whenever clinically appropriate.
Is Interventional Radiology a Better Option Than Surgery?
Interventional radiology can be a valuable uterus-sparing alternative to surgery for appropriately selected women with symptomatic fibroids and some cases of adenomyosis.
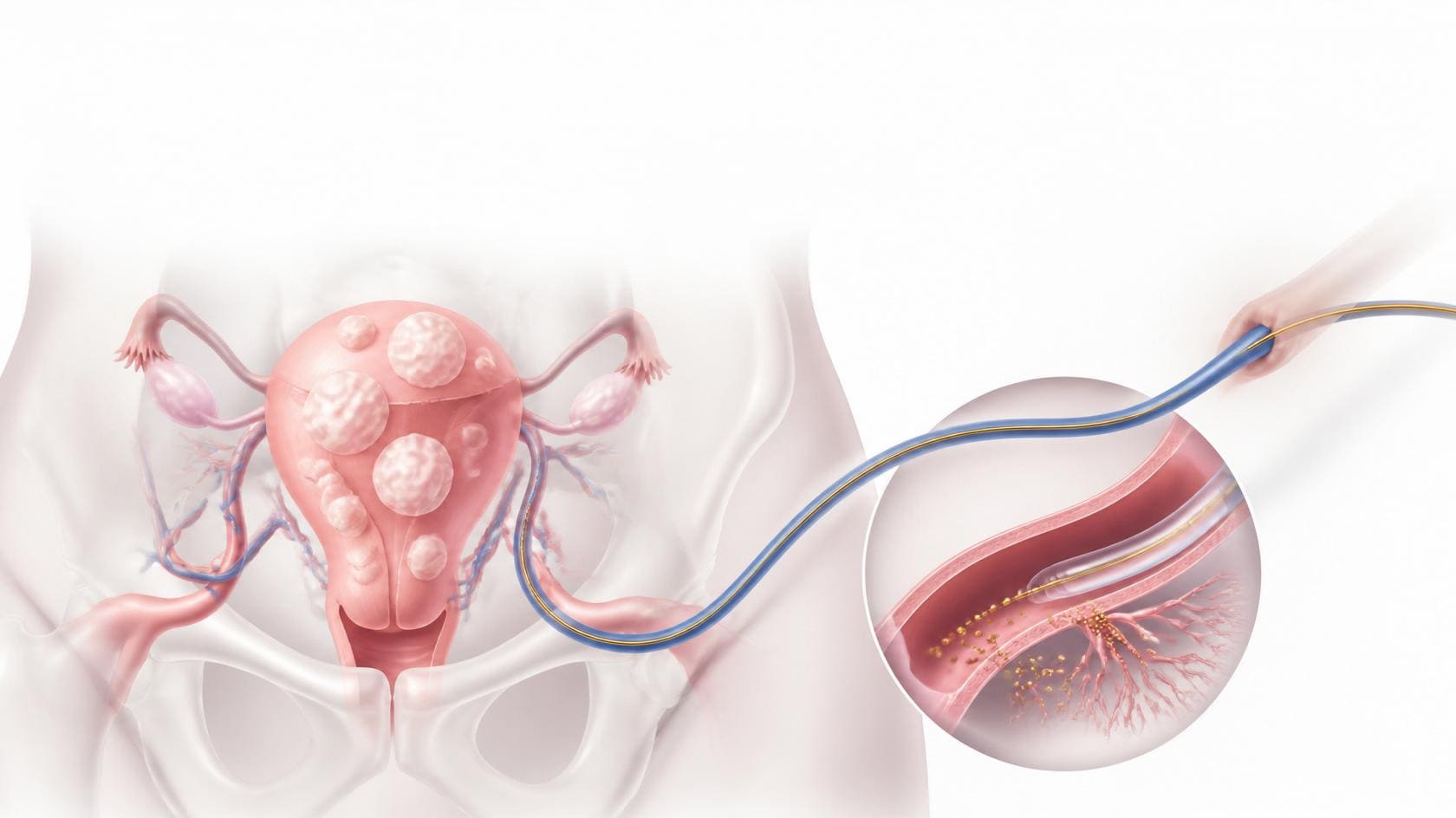
Uterine artery embolization is a minimally invasive procedure that reduces blood flow to targeted uterine tissue. For fibroids, this can shrink growths and improve heavy bleeding, pelvic pressure, and bulk-related symptoms without removing the uterus.
For adenomyosis, embolization-based treatment may be considered in selected patients after specialist assessment. The aim is to reduce the abnormal blood supply contributing to symptoms while avoiding open surgery.
Interventional radiology is not automatically preferable for every woman. The best option depends on the diagnosis, size and type of fibroids, extent of adenomyosis, future pregnancy plans, prior treatments, imaging findings, and overall health.
In Cairo and London, Dr. Samir Abdel Ghaffar provides a detailed consultation process that reviews imaging and symptoms before recommending an appropriate minimally invasive treatment pathway. This individualized approach helps avoid unnecessary surgical procedures when an image-guided option is suitable.
Can You Get Pregnant After Uterine Artery Embolization?
Which Is Worse: Adenomyosis or Fibroids?
Neither condition is universally worse because severity depends on symptoms, anemia, fertility concerns, and how much the condition affects daily life.
Adenomyosis may feel more severe for women whose main problem is debilitating cramps, chronic pelvic pain, painful intercourse, or diffuse uterine tenderness. Fibroids may be more disruptive when they cause major heavy bleeding, a large abdominal mass, frequent urination, constipation, or fertility problems.
Some women have minimal symptoms despite large fibroids or extensive adenomyosis. Others have intense symptoms from smaller abnormalities. The main issue is not the label alone but the real impact on health, anemia, work, sleep, relationships, and reproductive plans.
Doctors recommend seeking evaluation when periods become heavier, pain becomes progressively worse, or symptoms interfere with normal activities. Severe bleeding should never be normalized simply because a woman has experienced it for years.
Can Adenomyosis and Fibroids Occur Together?
Yes, adenomyosis and fibroids can occur together, and this combination can intensify heavy bleeding, pelvic pain, and diagnostic confusion.
Adenomyosis and fibroids share some hormone-related risk factors and often develop during reproductive years. Their Similar Symptoms can make it difficult to determine which condition is the main cause of heavy bleeding or pain.
When both are present, treatment should address the complete uterine picture rather than focusing on one finding alone. For example, a woman may have a submucosal fibroid causing heavy bleeding and diffuse adenomyosis contributing to severe cramps.
Advanced ultrasound and MRI can help map the different conditions and determine whether a minimally invasive, medical, surgical, or combined treatment plan is most appropriate. Research articles increasingly support personalized treatment instead of a one-size-fits-all approach.
What Is the Difference Between Adenomyosis vs Endometriosis?
Adenomyosis is endometrial-like tissue within the uterine muscle, while endometriosis occurs when similar tissue develops outside the uterus.
In adenomyosis, the abnormal tissue is located inside the womb wall. In endometriosis, lesions may occur on the ovaries, fallopian tubes, pelvic lining, bowel, bladder, or other pelvic structures.
Both conditions can cause painful periods, pain during intercourse, chronic pelvic pain, and fertility concerns. However, endometriosis may also cause bowel symptoms, painful bowel movements, urinary pain during menstruation, or pain that extends beyond the period itself.
Adenomyosis often causes a bulky, tender uterus and heavy menstrual bleeding. Endometriosis may not be visible on routine ultrasound, especially when lesions are superficial. This is why careful clinical evaluation remains essential even when imaging does not show a large abnormality.
Adenomyosis vs Fibroids vs Endometriosis: How Do They Compare?
Adenomyosis affects the uterine wall, fibroids are muscle growths in or around the uterus, and endometriosis develops outside the uterus.
| Condition | Location | Typical symptoms | Common imaging approach |
| Adenomyosis | Within the muscle of the uterus | Heavy painful periods, pelvic tenderness, cramps | Transvaginal ultrasound, MRI |
| Fibroids | Inside, within, or outside the uterus | Heavy bleeding, pressure, urinary symptoms, bloating | Ultrasound, MRI |
| Endometriosis | Outside the uterus | Pelvic pain, painful sex, bowel or bladder symptoms, infertility | Ultrasound, MRI, laparoscopy in selected cases |
These are different conditions, but a woman can have more than one at the same time. This overlap explains why symptoms may persist even after treatment for one disorder.
Hormones affect all three conditions, but their causes and treatment strategies are not identical. A complete diagnosis should consider the uterine lining, muscle wall, ovaries, pelvis, bleeding pattern, and fertility priorities.
Quick Facts and Common Misconceptions
Adenomyosis and fibroids are benign conditions, but they can still cause serious symptoms such as anemia, severe pain, and reduced quality of life.
Quick Facts
- Adenomyosis and fibroids are not the same condition.
- Both can cause heavy menstrual bleeding and anemia.
- Fibroids are distinct solid growths; adenomyosis is tissue within the uterine muscle.
- Ultrasound is often the first diagnostic test.
- MRI may help when ultrasound is inconclusive.
- Both conditions may occur with endometriosis.
- Not every fibroid requires treatment.
- Minimally invasive treatment may be possible for suitable patients.
Common Misconceptions
“All fibroids require surgery.”
Many fibroids do not require treatment if they cause no symptoms. When treatment is needed, medication, uterine artery embolization, hysteroscopic procedures, and other options may be considered before major surgery.
“Adenomyosis only affects older women.”
Although adenomyosis is commonly diagnosed in women in their 30s and 40s, it can affect younger women as well.
“Heavy periods are normal after childbirth or with age.”
Heavy bleeding should be assessed, especially if it causes anemia, clots, dizziness, fatigue, or major disruption to daily life.
“Vitamin deficiency causes fibroids.”
No vitamin deficiency has been confirmed as a direct cause of fibroids. Vitamin D levels and other factors are being studied, but women should not rely on supplements instead of proper diagnosis and treatment.
“LUPRON DEPOT permanently cures fibroids.”
LUPRON DEPOT may temporarily suppress hormone activity in selected situations, but symptoms and fibroid growth can return after treatment stops.
When Should You See a Doctor Immediately?
Seek urgent medical care for very heavy bleeding, fainting, chest pain, shortness of breath, severe sudden pelvic pain, fever, or possible pregnancy-related bleeding.
Book a timely specialist assessment if you experience periods lasting longer than usual, frequent flooding, large blood clots, worsening pelvic pain, pressure symptoms, infertility, or new bleeding between periods. These symptoms may be caused by fibroids, adenomyosis, endometriosis, hormonal abnormalities, polyps, or other uterine conditions.
Immediate assessment is particularly important if you feel dizzy, faint, extremely weak, pale, breathless, or experience palpitations, as these may indicate significant blood loss or anemia. New pelvic pain after menopause, unexplained weight loss, or a rapidly enlarging abdominal mass also requires medical evaluation.
Dr. Samir Abdel Ghaffar offers specialist interventional radiology assessment in Cairo and London for women seeking a minimally invasive pathway for uterine fibroids and selected adenomyosis cases.
Frequently Asked Questions
The following FAQs provide clear answers to common questions about adenomyosis, fibroids, imaging, and treatment options.
Can fibroids be misdiagnosed as adenomyosis?
Yes. Focal adenomyosis can resemble fibroids on ultrasound, particularly when there is a localized adenomyoma. MRI and specialist review may help distinguish between them.
Is adenomyosis more painful than fibroids?
Adenomyosis is often associated with stronger menstrual cramps and diffuse pelvic pain, while fibroids more often cause pressure symptoms and heavy bleeding. Either condition can be severe.
What are the first signs of adenomyosis?
Early signs may include heavier periods, worsening cramps, pelvic heaviness, painful intercourse, and a tender or enlarged uterus. Symptoms vary between women.
Is adenomyosis a serious problem?
Adenomyosis is benign, but it can seriously affect quality of life through heavy bleeding, anemia, chronic pain, fertility concerns, and emotional stress.
What test confirms fibroids?
Pelvic ultrasound is usually the first test used to identify fibroids. MRI may be recommended for complex cases or treatment planning.
What does a gynecologist do for adenomyosis?
A gynecologist assesses symptoms, performs examination and imaging, checks for anemia, discusses medical therapy, and refers for surgical or interventional radiology treatment when appropriate.
Which vitamin deficiency causes fibroids?
No vitamin deficiency is proven to directly cause fibroids. Vitamin D deficiency has been studied as a possible association, but it is not an established cause.
Can adenomyosis look like fibroids on ultrasound?
Yes. Adenomyosis, especially focal adenomyosis, can resemble fibroids on ultrasound. MRI may help clarify the diagnosis when imaging findings are uncertain.
Contact Dr. Samir Abdel Ghaffar
Dr. Samir Abdel Ghaffar is a Consultant Interventional Radiologist offering advanced image-guided treatment options for uterine fibroids and selected adenomyosis cases.
🇬🇧 London – United Kingdom
Clinic Number: +44 20 8144 2266
WhatsApp: +44 7377790644
🇪🇬 Cairo – Egypt
Booking Number: +20 1000 881336
WhatsApp: +20 1000 881336
Medical References
- American College of Obstetricians and Gynecologists. Uterine Fibroids: Frequently Asked Questions.
- National Institute for Health and Care Excellence. Heavy Menstrual Bleeding: Assessment and Management.
- National Institute for Health and Care Excellence. Uterine Artery Embolisation for Treating Adenomyosis.
- Society of Obstetricians and Gynaecologists of Canada. Diagnosis and Management of Adenomyosis Clinical Practice Guideline.
- U.S. Food and Drug Administration. LUPRON DEPOT Prescribing Information and Safety Information.
- Vannuccini S, Petraglia F. Recent advances in understanding and managing adenomyosis.
- American College of Obstetricians and Gynecologists. Abnormal Uterine Bleeding.
“The information in this article is for educational purposes only and does not replace consultation with a qualified physician. Every medical condition is unique and requires individual evaluation. Do not make any medical decisions based solely on this content.”

